

Abstract
The clinical course of WM widely differs among patients, with some manifesting symptoms as a consequence of the monoclonal IgM component or lymphoma infiltration. IgM-MGUS is generally asymptomatic while, in some cases, paraprotein-related manifestations may occur. Patients with IgM-MGUS should perform a regular follow-up as they are at risk of developing WM or other B-cell lymphoproliferative disorders (1.5-2% per year).
Although WM typically afflicts the elderly, there are no studies addressing the impact of ECOG performance status and comorbidities on patients' outcome. Furthermore, to our knowledge health-related quality of life (HRQOL) has never been evaluated in this category. The aim of this study is to analyze the impact of diagnosis and patients' characteristics on quality of life.
From October 2017, HRQOL was assessed in 103 patients (37 WM with previous or ongoing treatment [tWM]; 29 asymptomatic MW [aWM]; 37 IgM-MGUS) by the administration of EORTC QLQ-C30, HADS, FACT-GOG neurotoxicity and EQ-5D-5L questionnaires. Demographic anamnestic and disease-related data were also collected for each patient. The same questionnaires continue to be administered every 6 months for 3 years, in order to capture changes in HRQOL over time.
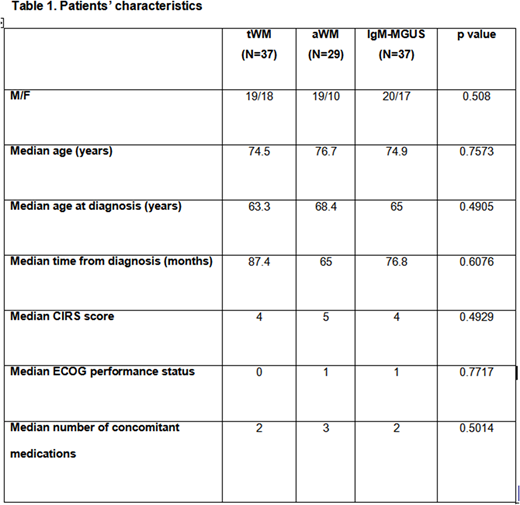
Patients features are reported in table 1. No significant differences in terms of age, sex distribution, age at diagnosis, months from diagnosis, ECOG performance status, CIRS or number of concomitant medications, were detected among the 3 groups (table 1).
As regards CIRS, the organ systems mainly involved resulted: vascular and genitourinary for tWM, genitourinary for aWM and vascular, respiratory and genitourinary for IgM-MGUS.
Among the 3 groups no statistical differences were reported when analyzing: EORTC QLQ-C30 global health status, functional scales (physical, role, emotional, cognitive and social functioning) and symptoms scale, EQ-5D VAS score, HADS anxiety and depression scores or FACT-GOG neurotoxicity score.
Males had higher global health status and emotional function when compared to females both in IgM-MGUS and WM patients. Higher CIRS score and ECOG status negatively impacted on global health status, physical function, EQ-5D VAS score and anxiety both in WM and IgM-MGUS. WM patients with longer time from diagnosis showed a significantly worse emotional function.
Patients-reported symptoms that could be referred to peripheral neuropathy (PN, 39 patients) resulted the only significant parameter negatively impacting on HRQOL (global health status, functional and symptoms scales according to EORTC QLQ-C30 and EQ-5D VAS score) and also affecting HADS anxiety score.
The diagnosis of PN was confirmed by neurologic tests only in 16/39 subjects that, compared with the rest of the population, showed older age (p .019), older age at diagnosis (p . 015) and higher ECOG status (p .005). In these patients, EORTC QLQ-C30 detected a reduced cognitive function (p .0031), while HADS a greater perception of anxiety (p .0015). No differences were recorded for EQ-5D VAS score or HADS depression scale.
In conclusion, in our series diagnosis per se didn't seem to affect HRQOL which was negatively influenced by high ECOG status and comorbidities. Emotional function meaningfully deteriorated as the time lapse from diagnosis became longer. Quality of life was significantly altered in patients reporting symptoms of PN and this was confirmed by all the questionnaires. Longer follow up is needed to confirm these preliminary data.
Montillo:Roche: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria; AbbVie: Consultancy, Honoraria, Speakers Bureau; Gilead: Consultancy, Honoraria, Speakers Bureau. Tedeschi:Janssen: Consultancy, Speakers Bureau; AbbVie: Consultancy; Gilead: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal